
What Sets Physically Active Rural Communities Apart from Less Active Ones? A Comparative Case Study of Three US Counties

 ,
,  , ,
, ,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments and Data Collection
Researcher Reflexivity
2.3. Analysis
2.3.1. Codebook Development
2.3.2. The Community Capital Framework
2.3.3. Transcript Coding
2.3.4. Member Checking
3. Results
3.1. Cultural Capital
I used to get a lot of exercise just from some of the work I did, construction, that thing. Probably, being in the Army and when I was a kid … I did a lot of stuff as a kid, did a lot of hunting and walking. And just probably built my body up enough to last a while. I don′t know how much longer it′s gonna last … But I had a feeling because of that exercise I got as a young guy and some of the employment that I chose, self-employment, that I just stayed pretty well healthy. Now I sit around too much, but that′s why I try and go play golf two or three times a week. And go to the football and basketball game.
I would say, with our little kids, they′re pretty active. The summer time and in the evenings, you′re gonna see kids on bikes, kids walking, kids hanging out playing, like back in the old days, whenever kids would go outside and play. There′s quite a bit of that. I mean, now of course, as you get older, our high school kids, not so much … our high schools kids are mostly involved in sports through the school … at least 50%, probably more between 60 and 70 are involved in athletics of some sort.
3.2. Human Capital
I just think that we [school system] lost some key funding, and they went to make some cuts. The people above my head are not as strong of a fitness and health people as I used to have here, including we got a new superintendent, we got a new curriculum director, we got three new principals.…I already broke them other ones in too…I don′t want to say I bullied them into it, but I persuaded them in a positive way to say, “Look, this is the best thing for all humans. If humans were meant to sit down, we′d be built a different way.” They′re not.
Some [shifts] are 8:00 [A.M.] to 8:00 [P.M.]…you know if they get a chance to work over, a lot of parents I know work over. They won′t know until that day starts, you know. And if they need to work over, they′ll work over… [because of that] we don′t have a lot of participation with hands on at the Boys and Girls Club with African American dads.
3.3. Social Capital
3.4. Organizational Capital
It [a worksite wellness program] went over well if it was in a group that was already established, but if I were to just market it through the newspaper, I mean, no one′s … It would have to be a group, like I′ve done it with teachers before at a school and they loved it because they were competing against other schools or the superintendent′s office or something like that, but I′ve not done a lot of physical activity education.
We have a board policy. If it′s a private individual the policy is much more strict, of course, because of liability reasons. You have to have a school district employee present, and there′s a deposit that must be left. There′s certain rules you have to follow when you′re here, for example, absolutely no alcoholic beverages or smoking. When it′s a community event we′re much more receptive to allowing things to happen because it′s promoting, it′s for the community, it′s for our kids. Let′s say a 30 year class reunion that wants to rent the cafeteria is a lot different than the community recreation wanting to play track and field on a Saturday for a tournament. There is a school district policy that mandates that.
3.5. Political Capital
I would love to have a gym kind of thing where we could bring people in and have equipment, moderate passive equipment… [for] recovering addicts. When you are in treatment, to have something like that, to be able to go and do bodybuilding, clearing your mind… When your body is healthy and your mind is active you just have a better life. And the ones around you have a better life.
3.6. Financial Capital
3.7. Natural Capital
3.8. Built Capital
We′re building a park back behind the [Extension office] facility, and that′s a start. If we had a real senior citizen′s center that could be used where we would have indoor pool which we could do water therapy. I would love to have a gym kind of thing where we could bring people in and have equipment, moderate passive equipment…
4. Discussion
4.1. Social Norms about PA
4.2. Quantity and Quality of Built Capital
4.3. Quantity and Track Record of Human and Organizational Capital
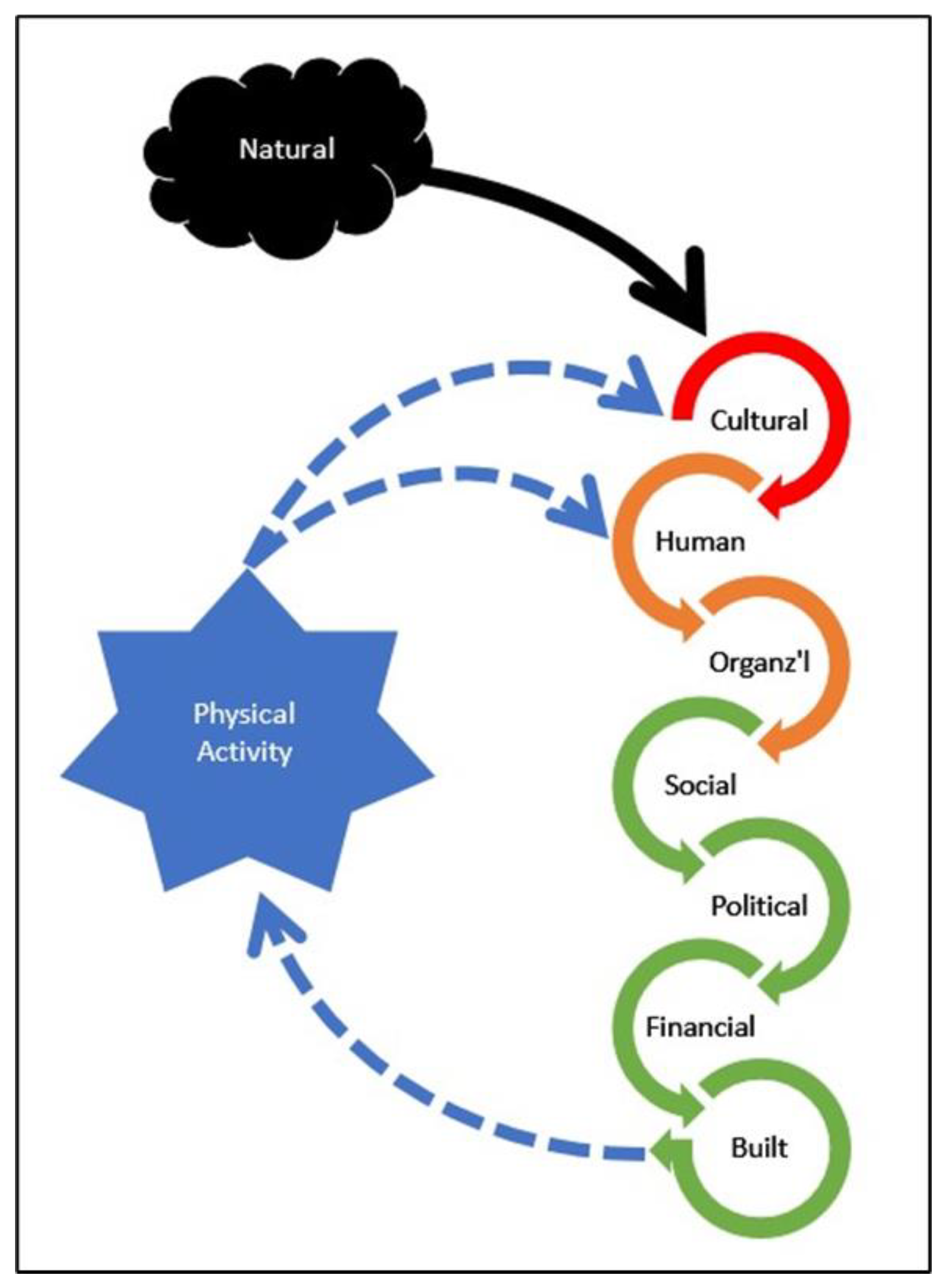
4.4. A Hypothetical Causal Model of How the Forms of Community Capital Create Physically Active Rural Communities
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef]
- United States Department of Health; Human Services Office of Disease Prevention and Health Promotion. Healthy People 2020; Office of Disease Prevention and Health Promotion: Rockville, MD, USA, 2012.
- Barker, D.C.; Gutman, M.A. Evaluation of Active Living Research: Ten Years of Progress in Building a New Field. Am. J. Prev. Med. 2014, 46, 208–215. [Google Scholar] [CrossRef]
- Sallis, J.F.; Cervero, R.; Ascher, W.; Henderson, K.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef] [Green Version]
- Hansen, A.Y.; Umstattd Meyer, M.R.; Lenardson, J.D.; Hartley, D. Built Environments and Active Living in Rural and Remote Areas: A Review of the Literature. Curr. Obes. Rep. 2015, 4, 484–493. [Google Scholar] [CrossRef] [PubMed]
- Frost, S.S.; Goins, R.T.; Hunter, R.H.; Hooker, S.P.; Bryant, L.L.; Kruger, J.; Pluto, D. Effects of the Built Environment on Physical Activity of Adults Living in Rural Settings. Am. J. Health Promot. 2010, 24, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Umstattd Meyer, M.R.; Moore, J.B.; Abildso, C.; Edwards, M.B.; Gamble, A.; Baskin, M.L. Rural Active Living: A Call to Action. J. Public Health Manag. Pract. 2016, 22, E11–E20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Guide to Community Preventive Services. Environmental and Policy Approaches to Increase Physical Activity: Creation of or Enhanced Access to Places for Physical Activity Combined with Informational Outreach Activities; The Community Guide: Atlanta, GA, USA, 2011; Volume 2011. [Google Scholar]
- United States Department of Agriculture Economic Research Service. Rural America at a Glance: 2019 Edition; USDA Economic Research Service: Washington, DC, USA, 2019.
- Emery, M.; Flora, C. Spiraling-Up: Mapping Community Transformation with Community Capitals Framework. Community Dev. 2006, 37, 19–35. [Google Scholar] [CrossRef]
- Eberhardt, M.S.; Pamuk, E.R. The Importance of Place of Residence: Examining Health in Rural and Nonrural Areas. Am. J. Public Health 2004, 94, 1682–1686. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Siahpush, M. Widening Rural–Urban Disparities in Life Expectancy, U.S., 1969–2009. Am. J. Prev. Med. 2014, 46, e19–e29. [Google Scholar] [CrossRef]
- Cosby, A.G.; McDoom-Echebiri, M.M.; James, W.; Khandekar, H.; Brown, W.; Hanna, H.L. Growth and Persistence of Place-Based Mortality in the United States: The Rural Mortality Penalty. Am. J. Public Health 2019, 109, 155–162. [Google Scholar] [CrossRef]
- Befort, C.A.; Nazir, N.; Perri, M.G. Prevalence of Obesity Among Adults From Rural and Urban Areas of the United States: Findings From NHANES (2005–2008). J. Rural Health 2012, 28, 392–397. [Google Scholar] [CrossRef] [Green Version]
- Trivedi, T.; Liu, J.; Probst, J.C.; Merchant, A.; Jones, S.; Martin, A.B. Obesity and obesity-related behaviors among rural and urban adults in the USA. Rural Remote Health 2015, 15. [Google Scholar] [CrossRef]
- Henley, S.J.; Anderson, R.N.; Thomas, C.C.; Massetti, G.M.; Peaker, B.; Richardson, L.C. Invasive cancer incidence, 2004–2013, and deaths, 2006–2015, in nonmetropolitan and metropolitan counties—United States. MMWR Surveill. Summ. 2017, 66, 1. [Google Scholar] [CrossRef] [PubMed]
- Carlson, S.A.; Whitfield, G.P.; Peterson, E.L.; Ussery, E.N.; Watson, K.B.; Berrigan, D.; Fulton, J.E. Geographic and Urban–Rural Differences in Walking for Leisure and Transportation. Am. J. Prev. Med. 2018, 55, 887–895. [Google Scholar] [CrossRef]
- Matthews, K.A.; Croft, J.B.; Liu, Y.; Lu, H.; Kanny, D.; Wheaton, A.G.; Cunningham, T.J.; Khan, L.K.; Caraballo, R.S.; Holt, J.B.; et al. Health-Related Behaviors by Urban-Rural County Classification—United States, 2013. MMWR. Surveill. Summ. 2017, 66, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Whitfield, G.P.; Carlson, S.A.; Ussery, E.N.; Fulton, J.E.; Galuska, D.A.; Petersen, R. Trends in Meeting Physical Activity Guidelines Among Urban and Rural Dwelling Adults—United States, 2008–2017. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 513–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umstattd Meyer, M.R.; Perry, C.K.; Sumrall, J.C.; Patterson, M.S.; Walsh, S.M.; Clendennen, S.C.; Hooker, S.P.; Evenson, K.R.; Goins, K.V.; Heinrich, K.M.; et al. Physical Activity-Related Policy and Environmental Strategies to Prevent Obesity in Rural Communities: A Systematic Review of the Literature, 2002–2013. Prev. Chronic Dis. 2016, 13, E03. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnidge, E.K.; Radvanyi, C.; Duggan, K.; Motton, F.; Wiggs, I.; Baker, E.A.; Brownson, R.C. Understanding and Addressing Barriers to Implementation of Environmental and Policy Interventions to Support Physical Activity and Healthy Eating in Rural Communities. J. Rural Health 2013, 29, 97–105. [Google Scholar] [CrossRef] [Green Version]
- Handler, A.; Issel, M.; Turnock, B. A Conceptual Framework to Measure Performance of the Public Health System. Am. J. Public Health 2001, 91, 1235–1239. [Google Scholar] [CrossRef]
- Dwyer-Lindgren, L.; Freedman, G.; Engell, R.E.; Fleming, T.D.; Lim, S.S.; Murray, C.J.L.; Mokdad, A.H. Prevalence of physical activity and obesity in US counties, 2001–2011: A road map for action. Popul. Health Metr. 2013, 11, 7. [Google Scholar] [CrossRef] [Green Version]
- Marsh, D.R.; Schroeder, D.G. The Positive Deviance Approach to Improve Health Outcomes: Experience and Evidence from the Field—Preface. Food Nutr. Bull. 2002, 23, 3–6. [Google Scholar] [CrossRef] [Green Version]
- Bolles, K.; Speraw, C.; Berggren, G.; Lafontant, J.G. Ti Foyer (Hearth) Community-Based Nutrition Activities Informed by the Positive Deviance Approach in Leogane, Haiti: A Programmatic Description. Food Nutr. Bull. 2002, 23, 9–15. [Google Scholar] [CrossRef]
- Mackintosh, U.A.T.; Marsh, D.R.; Schroeder, D.G. Sustained Positive Deviant Child Care Practices and Their Effects on Child Growth in Viet Nam. Food Nutr. Bull. 2002, 23, 16–25. [Google Scholar] [CrossRef]
- Lapping, K.; Schroeder, D.; Marsh, D.; Albalak, R.; Jabarkhil, M.Z. Comparison of a Positive Deviant Inquiry with a Case-Control Study to Identify Factors Associated with Nutritional Status among Afghan Refugee Children in Pakistan. Food Nutr. Bull. 2002, 23, 26–33. [Google Scholar] [CrossRef]
- Buettner, D. The Blue Zones: 9 Lessons for Living Longer from the People Who’ve Lived the Longest; National Geographic: Washington, DC, USA, 2008; p. 277. [Google Scholar]
- Poulain, M.; Herm, A.; Pes, G. The Blue Zones: Areas of exceptional longevity around the world. Vienna Yearb. Popul. Res. 2013, 11, 87–108. [Google Scholar] [CrossRef]
- Creswell, J.W.; Poth, C.N. Qualitative Inquiry and Research Design: Choosing among Five Approaches; SAGE Publications: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Yin, R.K. Case Study Research: Design and Methods, 5th ed.; SAGE Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Thomas, D.R. A General Inductive Approach for Analyzing Qualitative Evaluation Data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Bradley, E.H.; Curry, L.A.; Devers, K.J. Qualitative Data Analysis for Health Services Research: Developing Taxonomy, Themes, and Theory. Health Serv. Res. 2007, 42, 1758–1772. [Google Scholar] [CrossRef] [Green Version]
- Flora, C.B.; Flora, J.L. Rural Communities: Legacy and Change, 3rd ed.; Westview Press: Boulder, CO, USA, 2007. [Google Scholar]
- Roseland, M. Toward Sustainable Communities: Solutions for Citizens and Their Governments, 4th ed.; New Society Publishers: Gabriola Island, BC, Canada, 2012. [Google Scholar]
- Stout, M. Pursuing Community Change through Radically Democratic Practice. In Reframing Nonprofit Organizations: Democracy, Inclusion, and Social Change, Eikenberry, A.M., Mirabella, R.M., Sandberg, B., Eds.; Melvin & Leigh Publishers: Irvine, CA, USA, 2019; pp. 106–123. [Google Scholar]
- Flora, C.B.; Flora, J.L.; Gasteyer, S.P. Rural Communities: Legacy + Change, 4th ed.; Westview Press: Boulder, CO, USA, 2016. [Google Scholar]
- Kretzmann, J.P.; McKnight, J.L. Introduction. In Building Communities from the Inside Out: A Path Toward Finding and Mobilizing a Community’s Assets; Asset-Based Community Development Institute: Chicago, IL, USA, 1993. [Google Scholar]
- Secretary’s Advisory Committee on Health Promotion and Disease Prevention. Healthy People 2020: An Opportunity to Address the Societal Determinants of Health in the United States; Office of Disease Prevention and Health Promotion: Rockville, MD, USA, 2010.
- Holden, M. Revisiting the local impact of community indicators projects: Sustainable Seattle as prophet in its own land. Appl. Res. Qual. Life 2006, 1, 253–277. [Google Scholar] [CrossRef]
- Kolodinsky, J.; Roche, E.; DeSisto, T.; Sawyer, W.; Propen, D. Understanding quality of life in a northern, rural climate. Community Dev. 2013, 44, 161–172. [Google Scholar] [CrossRef]
- Lowe, M.; Whitzman, C.; Badland, H.; Davern, M.; Aye, L.; Hes, D.; Butterworth, I.; Giles-Corti, B. Planning healthy, liveable and sustainable cities: How can indicators inform policy? Urban Policy Res. 2015, 33, 131–144. [Google Scholar] [CrossRef]
- Perrings, C. Resilience in the dynamics of economy-environment systems. Environ. Resour. Econ. 1998, 11, 503–520. [Google Scholar] [CrossRef]
- Schrock, G. Connecting people and place prosperity: Workforce development and urban planning in scholarship and practice. J. Plan. Lit. 2014, 29, 257–271. [Google Scholar] [CrossRef] [Green Version]
- Roseland, M.; Spiliotopoulou, M.; Stout, M. Toward Sustainable Communities: Solutions for Citizens and Their Governments, 5th ed.; New Society Publishers: Gabriola Island, BC, Canada, 2022; in press. [Google Scholar]
- Centers for Disease Control and Prevention (CDC); National Center for Chronic Diseases Prevention and Health Promotion; Division of Nutrition, Physical Activity and Obesity. A Data Users Guide to the BRFSS Physical Activity Questions: How to Assess the 2008 Physical Activity Guidelines for Americans; Centers for Disease Control and Prevention (CDC): Atlanta, GA, USA, 2013.
- Corbin, C.B. Physical Activity for Everyone: What Every Educator Should Know About Promoting Lifelong Physical Activity. J. Teach. Phys. Educ. 2002, 21, 128. [Google Scholar] [CrossRef]
- Sallis, J.F.; McKenzie, T.L. Physical Education’s Role in Public Health. Res. Q. Exerc. Sport 1991, 62, 124–137. [Google Scholar] [CrossRef] [PubMed]
- White, M.J.; Perrin, A.J.; Caren, N.; Perrin, E.M. Back in the Day: Nostalgia Frames Rural Residents’ Perspectives on Diet and Physical Activity. J. Nutr. Educ. Behav. 2020, 52, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Mayo Clinic. Hunting and Heart Attacks. Available online: Https://www.mayoclinichealthsystem.org/hometown-health/speaking-of-health/hunting-and-heart-attacks (accessed on 22 July 2021).
- Spangler-Murphy, E.; Krummel, D.A.; Morrison, N.; Gordon, P.M. Environmental perceptions related to physical activity in high- and low-risk counties. Health Promot. Pract. 2005, 6, 57–63. [Google Scholar] [CrossRef]
- Schulenkorf, N.; Siefken, K. Managing sport-for-development and healthy lifestyles: The sport-for-health model. Sport Manag. Rev. 2019, 22, 96–107. [Google Scholar] [CrossRef]
- Gardam, K.J.; Giles, A.R.; Rynne, S.; Hayhurst, L.M. A comparison of Indigenous sport for development policy directives in Canada and Australia. Aborig. Policy Stud. 2019, 7, 29–46. [Google Scholar] [CrossRef] [Green Version]
- Edwards, M.B. The role of sport in community capacity building: An examination of sport for development research and practice. Sport Manag. Rev. 2015, 18, 6–19. [Google Scholar] [CrossRef]
- Edwards, M.B.; Rowe, K. Managing sport for health: An introduction to the special issue. Sport Manag. Rev. 2019, 22, 1–4. [Google Scholar] [CrossRef]
- Whitfield, G.P.; Carlson, S.A.; Ussery, E.N.; Watson, K.B.; Berrigan, D.; Fulton, J.E. National-level environmental perceptions and walking among urban and rural residents: Informing surveillance of walkability. Prev. Med. 2019, 123, 101–108. [Google Scholar] [CrossRef]
- Chrisman, M.; Nothwehr, F.; Yang, G.; Oleson, J. Environmental influences on physical activity in rural Midwestern adults: A qualitative approach. Health Promot. Pract. 2015, 16, 142–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, T.; Eyler, A.A.; Tabak, R.G.; Valko, C.; Brownson, R.C. Opportunities for Promoting Physical Activity in Rural Communities by Understanding the Interests and Values of Community Members. J. Environ. Public Health 2017, 2017, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbert, A.S.; Duncan, D.D.; Beck, A.M.; Eyler, A.A.; Brownson, R.C. A Qualitative Study Identifying Barriers and Facilitators of Physical Activity in Rural Communities. J. Environ. Public Health 2019, 2019, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cherrington, A.; Ayala, G.X.; Elder, J.P.; Arredondo, E.M.; Fouad, M.; Scarinci, I. Recognizing the diverse roles of community health workers in the elimination of health disparities: From paid staff to volunteers. Ethn. Dis. 2010, 20, 189–194. [Google Scholar] [PubMed]
- Nichols, D.C.; Berrios, C.; Samar, H. Texas’ Community Health Workforce: From State Health Promotion Policy to Community-Level Practice. Available online: http://www.cdc.gov/pcd/issues/2005/nov/05_0059.htm (accessed on 22 July 2021).
- Ebinger, J.; Blyler, C.A.; Brettler, J.; Rader, F. Barbershop Management of Hypertension in the African American Population: Pitfalls and Opportunities for Extension to Other Underserved Communities. Curr. Cardiol. Rep. 2020, 22, 64. [Google Scholar] [CrossRef]
- Ferdinand, D.P.; Nedunchezhian, S.; Ferdinand, K.C. Hypertension in African Americans: Advances in community outreach and public health approaches. Prog. Cardiovasc. Dis. 2020, 63, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Sutton, V.; Hites, L.; Graham, J.; Karimi, M.; Dove, C.; Walls, T.; Wilson-Simpson, F.; McGuire, A.; Zhang, L.; Dobbs, T. Targeting Hypertension: Working with Rural Barbershops to Identify Hypertension and Encourage Treatment. J. Health Care Poor Underserved 2021, 32, 258–270. [Google Scholar] [CrossRef]
- Pate, R.R. A National Physical Activity Plan for the United States. J. Phys. Act. Health 2009, 6, S157–S158. [Google Scholar] [CrossRef] [Green Version]
- Bornstein, D.B.; Carnoske, C.; Tabak, R.; Maddock, J.; Hooker, S.P.; Evenson, K.R. Factors Related to Partner Involvement in Development of the US National Physical Activity Plan. J. Public Health Manag. Pract. 2013, 19, S8–S16. [Google Scholar] [CrossRef] [Green Version]
- Kraus, W.E.; Bittner, V.; Appel, L.; Blair, S.N.; Church, T.; Després, J.-P.; Franklin, B.A.; Miller, T.D.; Pate, R.R.; Taylor-Piliae, R.E.; et al. The National Physical Activity Plan: A Call to Action From the American Heart Association: A Science Advisory From the American Heart Association. Circulation 2015, 131, 1932–1940. [Google Scholar] [CrossRef]
- Rural Health Information Hub. Substance Abuse in Rural Areas. Available online: https://www.ruralhealthinfo.org/topics/substance-abuse (accessed on 11 October 2019).
- Lynch, W.J.; Peterson, A.B.; Sanchez, V.; Abel, J.; Smith, M.A. Exercise as a novel treatment for drug addiction: A neurobiological and stage-dependent hypothesis. Neurosci. Biobehav. Rev. 2013, 37, 1622–1644. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Wang, Y.; Wang, Y.; Li, R.; Zhou, C. Impact of Physical Exercise on Substance Use Disorders: A Meta-Analysis. PLoS ONE 2014, 9, e110728. [Google Scholar] [CrossRef] [Green Version]
- Leider, J.P.; Meit, M.; McCullough, J.M.; Resnick, B.; Dekker, D.; Alfonso, Y.N.; Bishai, D. The State of Rural Public Health: Enduring Needs in a New Decade. Am. J. Public Health 2020, 110, 1283–1290. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social Learning Theory; Prentice-Hall: Hoboken, NJ, USA, 1977.
- Bronfenbrenner, U. Toward an experimental ecology of human development. Am. Psychol. 1977, 32, 513–531. [Google Scholar] [CrossRef]
- Meadows, D.H. Thinking in Systems: A Primer; Chelsea Green Publishing: White River Junction, VT, USA, 2008. [Google Scholar]
- Carter, W.M.; Morse, W.C.; Brock, R.W.; Struempler, B. Improving Physical Activity and Outdoor Recreation in Rural Alabama Through Community Coalitions. Prev. Chronic Dis. 2019, 16, 6. [Google Scholar] [CrossRef]
- Wallace, H.S.; Franck, K.L.; Sweet, C.L. Community Coalitions for Change and the Policy, Systems, and Environment Model: A Community-Based Participatory Approach to Addressing Obesity in Rural Tennessee. Prev. Chronic Dis. 2019, 16, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, A.M.; Eyler, A.A.; Aaron Hipp, J.; King, A.C.; Tabak, R.G.; Yan, Y.; Reis, R.S.; Duncan, D.D.; Gilbert, A.S.; Serrano, N.H.; et al. A multilevel approach for promoting physical activity in rural communities: A cluster randomized controlled trial. BMC Public Health 2019, 19, 10. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | HPA 1 | HPA 2 | LPA |
|---|---|---|---|
| Population 1 | 10,497 | 4087 | 8865 |
| White, Non-Hispanic, % 3 | 78.0 | 42.8 | 68.8 |
| Black, Non-Hispanic, % 3 | 0 | 0.7 | 21.7 |
| Hispanic, % 3 | 18.9 | 55.5 ¢ | 6.7 |
| Female PAG prevalence, %, 2011 [23] | 56.0 | 49.9 | 39.6 |
| Male PAG prevalence, %, 2011 [23] | 59.5 | 56.8 | 44.7 |
| Population living in a rural area, % 1 | 100 | 100 | 100 |
| Rural-Urban Continuum Code (RUCC) 2¶ | 8 | 8 | 9 |
| Urban Influence Code (UIC) 2§ | 4 | 6 | 10 |
| Rural-Urban Commuting Area (RUCA; for each Census tract within the county) 2¥ | 10, 3 | 2 | 10, 10, 3 |
| Economy “type” 2@ | Recreation | Farming | Non-specialized |
| Median household income, USD 3 | $56,573 | $48,516 | $29,426 |
| Population below the poverty level, % 3 | 9.7 | 10.6 | 26.6 |
| Interviewee Code | Sex | Age Group | Race | Title | Interview Length |
|---|---|---|---|---|---|
| HPA1.1 | Female | 40–49 | White | Cooperative Extension County Coordinator | 44:09 |
| HPA1.2 | Male | 50–59 | White | Cooperative Extension Agent | 5:10 |
| HPA1.3 | Male | 40–49 | White | High School Coach/Physical Education Teacher | 32:03 |
| HPA1.4 | Female | 50–59 | White | Cooperative Extension Administrative Assistant | 2:40 |
| HPA2.1 | Female | 40–49 | White | Cooperative Extension County Coordinator | 13:10 |
| HPA2.2 | Female | 40–49 | White | High School Principal/Superintendent | 14:10 |
| HPA2.3 | Male | 70+ | White | Newspaper Publisher | 18:40 |
| LPA.1 | Female | 50–59 | White | Cooperative Extension County Coordinator | 15:24 |
| LPA.2 | Female | 60–69 | White | County Judge | 42:28 |
| LPA.3 | Female | 50–59 | White | High School Principal | 26:27 |
| LPA.4 | Female | 40–49 | White | School District, Counselor | 31:19 |
| LPA.5 | Female | 70+ | White | Extension Programming Volunteer with Seniors | 26:03 |
| LPA.6 | Female | 40–49 | White | Chamber of Commerce Staff Member | 11:56 |
| LPA.7 | Male | 50–59 | Black | High School Teacher/Boys and Girls Club Director | 30:21 |
| Form of Capital | Original Definition | Operational Definition |
|---|---|---|
| Cultural Capital | Cultural capital reflects the way people “know the world” and how they act within it, as well as their traditions and language. Cultural capital influences what voices are heard and listened to, which voices have influence in what areas, and how creativity, innovation, and influence emerge and are nurtured. Hegemony privileges the cultural capital of dominant groups. | The way people “know the world” that hinders or fosters how they act within it (i.e., cultural beliefs and traditions influence individual decisions about engaging in PA), as well as their language about and attitudes toward PA. Cultural capital influences whose voices are heard and which voices have influence in what areas, and how creativity, innovation, and influence emerge and are nurtured. Hegemony privileges the cultural capital of dominant groups. |
| Human Capital | Human capital is understood to include the skills and abilities of people to develop and enhance their resources and to access outside resources and bodies of knowledge in order to increase their understanding, to identify promising practices, and to access data for community-building. Human capital addresses the leadership’s ability to “lead across differences”, to focus on assets, to be inclusive and participatory, and to act proactively in shaping the future of the community or group. | The skills and physical abilities of people to develop and access outside resources and bodies of knowledge about PA in order to increase their understanding and identify promising practices. Human capital addresses the leadership’s ability to “lead across differences”, to focus on assets, to be inclusive and participatory, and to act proactively in shaping the future of the PA of the community or group that they have influence over. It also includes the facilitators of and barriers to using skills and abilities to affect community level PA (e.g., time). |
| Social Capital | Social capital reflects the connections among people and organizations or the social “glue” to make things, positive or negative, happen. Bonding social capital refers to those close redundant ties that build community cohesion. Bridging social capital involves loose ties that bridge among organizations and communities. | The connections among people and organizations or the social “glue” to make things happen that increase community PA level. Bonding social capital refers to close ties that build community cohesion. Bridging social capital involves loose ties that bridge across social groups, organizations, and communities. |
| Organizational Capital [36] (p. 113) | The structure, policies, plans, and track record of existing groups (informal groups, organizations, and networks). | The structure, policies, plans, and track record of existing groups (informal groups, organizations, and networks) and their ability to collaborate in supporting PA. |
| Political Capital | Political capital reflects access to power, organizations, resources, and power brokers. Political capital also refers to the ability of people to find their own voice and to engage in actions that contribute to the well-being of their community. | Community political power, influence, and access to power brokers at local, county, state, and federal levels who support PA. |
| Financial Capital | Financial capital refers to the financial resources available to invest in community capacity-building, to underwrite the development of businesses, to support civic and social entrepreneurship, and to accumulate wealth for future community development. | Financial resources available to invest in programs and infrastructure that support PA. |
| Natural Capital | Natural capital refers to those assets that abide in a particular location, including weather, geographic isolation, natural resources, amenities, and natural beauty. Natural capital shapes the cultural capital connected to place. | Those assets that exist in a particular location without human intervention (i.e., not parks) that either foster or hinder community level PA, including weather, topography, natural resources, and natural beauty. Natural capital influences the cultural capital connected to place. |
| Built Capital | Built capital includes the infrastructure supporting these activities. | Built capital includes the infrastructure supporting PA activities, including the accessibility to and presence of parks. A sense of personal safety is necessary for its use. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abildso, C.G.; Perry, C.K.; Jacobs, L.; Umstattd Meyer, M.R.; McClendon, M.; Edwards, M.B.; Roemmich, J.N.; Ramsey, Z.; Stout, M. What Sets Physically Active Rural Communities Apart from Less Active Ones? A Comparative Case Study of Three US Counties. Int. J. Environ. Res. Public Health 2021, 18, 10574. https://doi.org/10.3390/ijerph182010574
Abildso CG, Perry CK, Jacobs L, Umstattd Meyer MR, McClendon M, Edwards MB, Roemmich JN, Ramsey Z, Stout M. What Sets Physically Active Rural Communities Apart from Less Active Ones? A Comparative Case Study of Three US Counties. International Journal of Environmental Research and Public Health. 2021; 18(20):10574. https://doi.org/10.3390/ijerph182010574
Chicago/Turabian StyleAbildso, Christiaan G., Cynthia K. Perry, Lauren Jacobs, M. Renée Umstattd Meyer, Megan McClendon, Michael B. Edwards, James N. Roemmich, Zachary Ramsey, and Margaret Stout. 2021. "What Sets Physically Active Rural Communities Apart from Less Active Ones? A Comparative Case Study of Three US Counties" International Journal of Environmental Research and Public Health 18, no. 20: 10574. https://doi.org/10.3390/ijerph182010574